The Challenge of Isolated Amniotic Fluid Volume Deviations
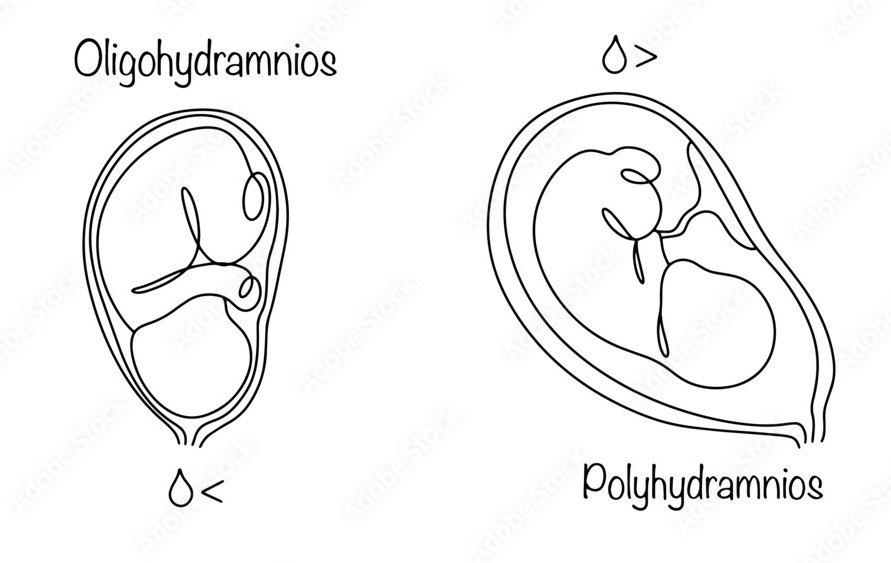
Amniotic fluid volume (AFV) is a primary marker used to assess fetal well-being during antenatal ultrasound surveillance. While an abnormal fluid volume frequently signals underlying maternal, fetal, or placental pathologies, encountering an isolated abnormality—where fetal anatomy, growth, and maternal health markers appear completely normal—is remarkably common yet highly contentious in clinical practice. In the United Kingdom, isolated oligohydramnios affects up to 5% of pregnancies, while isolated polyhydramnios is identified in up to 2%. Managing these cases requires a careful balance between avoiding unnecessary iatrogenic interventions and mitigating genuine perinatal risks.
The Measurement Debate and the “AFI < 8” Tendency
The clinical diagnosis of abnormal volume hinges on ultrasound metrics, primarily the single deepest vertical pocket (SDVP) and the four-quadrant amniotic fluid index (AFI). Landmark data, including a 2008 Cochrane systematic review and the 2015 multicenter SAFE trial, have demonstrated that the use of AFI significantly increases the diagnosis of oligohydramnios without improving perinatal outcomes, leading to higher rates of unnecessary inductions of labor. Consequently, SDVP has emerged as the preferred method for assessing fluid volume.
Despite the strict criteria defining oligohydramnios as an AFI < 5 cm or an SDVP < 2 cm, there is a strong and pervasive clinical tendency in many obstetric units to tag or manage a pregnancy as oligohydramnios when the AFI is less than 8 cm. This “borderline low” threshold often triggers heightened clinical anxiety and prompts reflexive diagnostic labeling. Clinicians frequently interpret an AFI between 5 cm and 8 cm as an early warning sign of evolving placental insufficiency, even when fetal biometry and Doppler indices are reassuring. This conservative approach contributes directly to the diagnostic inflation highlighted by the SAFE trial, frequently steering low-risk patients into pathways of intensive surveillance or expedited delivery without clear evidence of clinical benefit.
Clinical Scenarios
Scenario 1: The Overdiagnosis of Oligohydramnios at Term
- Patient Presentation: A 39-week asymptomatic multiparous patient undergoes an ultrasound scan for a clinical suspicion of unstable lie. The ultrasound confirms a stable cephalic presentation with normal fetal anatomy and a regular growth trajectory at the 50th percentile. However, the four-quadrant AFI is measured at 6.2 cm. The clinician records a diagnosis of “isolated oligohydramnios” and initiates a discussion regarding induction of labor.
- Clinical Analysis: This scenario illustrates the classic diagnostic inflation seen when applying an informal “AFI < 8 cm” threshold. By strict criteria, an AFI of 6.2 cm does not meet the definition for oligohydramnios (which requires an AFI < 5 cm or SDVP < 2 cm). As demonstrated by the SAFE trial, labeling this patient with oligohydramnios increases the likelihood of an emergency operative delivery or an induction with an unfavorable cervix, without delivering any quantifiable benefit to the neonate. An evidence-based approach involves re-evaluating the fluid using the SDVP method; if the SDVP is ≥ 2 cm, the fluid volume should be classified as normal, thereby avoiding unnecessary intervention while continuing routine care or standard post-dates surveillance.
Scenario 2: The Ambiguity of Third-Trimester Polyhydramnios
- Patient Presentation: A 36-week primiparous patient undergoes an ultrasound following an accelerated symphysis-fundal height measurement. The scan reveals an SDVP of 9.5 cm and an AFI of 27 cm, indicating mild-to-moderate polyhydramnios. A comprehensive structural survey is normal, and an oral glucose tolerance test (OGTT) rules out gestational diabetes.
- Clinical Analysis: With a normal anatomical survey and negative diabetic screening, this case satisfies the criteria for idiopathic or isolated polyhydramnios, which represents 60% to 70% of all polyhydramnios cases. The primary clinical challenge here is the known correlation between polyhydramnios and macrosomia that may not be fully detected on antenatal biometry. Furthermore, even when apparently isolated, there remains a baseline risk of underlying genomic or structural anomalies that only become apparent after birth. Management must be guided by severity: for mild cases, major organizations like ACOG advise against altering standard management, whereas guidelines like NICE mandate continuous cardiotocography (CTG) during labor due to risks such as cord prolapse or mechanical dystocia.

Evidence-Based Management Strategies
Isolated Polyhydramnios
When dealing with a confirmed diagnosis of isolated polyhydramnios (SDVP ≥ 8 cm or AFI ≥ 25 cm), investigation begins with a detailed history, physical assessment, diabetes screening, and an infection screen (TORCH). If these investigations are negative, management depends entirely on the severity of the fluid accumulation:
- Mild Polyhydramnios: Typically represents a benign course. There is no robust evidence demonstrating that early induction of labor improves outcomes, and many guidelines suggest managing expectantly.
- Moderate Polyhydramnios: The risk of adverse outcomes increases with severity, though clear thresholds remain poorly defined due to confounding factors like macrosomia. A pragmatic approach involves offering induction of labor from 40 weeks of gestation after a comprehensive discussion of risks and benefits.
- Severe Polyhydramnios: This carries a significant risk of maternal and fetal complications, alongside a 10% risk of an underlying neonatal genetic or structural abnormality. For these reasons, an expedited delivery via induction before 40 weeks is recommended, with the precise timing tailored to maternal symptoms and individual risk profiles.
- Therapeutic Interventions: Amnioreduction should be strictly reserved for patients experiencing severe maternal discomfort or respiratory distress, given the high rate of fluid reaccumulation and associated risks of preterm labor or placental abruption.
Isolated Oligohydramnios
True isolated oligohydramnios is a diagnosis of exclusion established after definitively ruling out ruptured membranes, fetal growth restriction (FGR), congenital infections, and maternal hypertensive or renal disorders.
- Antenatal Surveillance: Both ACOG and NICE recommend implementing increased ultrasound surveillance and fetal monitoring to track well-being.
- Intrapartum Management: Continuous electronic fetal monitoring is essential because the lack of a fluid cushion increases the susceptibility to acute or repetitive umbilical cord compression, raising the risk of intrapartum distress and emergency operative delivery.
- Timing of Delivery: The optimal timing remains heavily debated. While some evidence indicates that early induction does not reduce perinatal mortality and can increase iatrogenic risks, there is a known association between isolated oligohydramnios and an increased incidence of undiagnosed small-for-gestational-age (SGA) infants discovered only postpartum. Consequently, a pragmatic and widely supported approach is to offer induction of labor at term to prevent late-gestation compromise.
Postnatal Considerations and Long-Term Implications
The management of isolated fluid abnormalities does not end at delivery. For pregnancies complicated by severe isolated polyhydramnios, childhood surveillance is justified due to a documented 4.5% to 10% risk of eventual genomic abnormality diagnoses, with Bartter syndrome being the most prevalent genetic variant identified. Conversely, for pregnancies marked by isolated oligohydramnios, emerging data indicate an elevated risk of recurrent placental-related disorders in subsequent pregnancies. This finding justifies implementing enhanced serial ultrasound growth monitoring in future gestations to ensure early detection of placental insufficiency.
References
-
Falola AO, Filby L, Timmons P, Alleemudder D. Management of isolated abnormal amniotic fluid volume in pregnancy. The Obstetrician & Gynaecologist 2026;28:41-50. https://doi.org/10.1111/tog.70021
-
Nabhan AF, Abdelmoula YA. Amniotic fluid index versus single deepest vertical pocket as a screening test for preventing adverse pregnancy outcome. Cochrane Database of Systematic Reviews 2008;(3):CD006593.
-
Kehl S, Schelkle A, Thomas A, et al. Single deepest vertical pocket or amniotic fluid index as evaluation test for predicting adverse pregnancy outcome (SAFE trial): a multicenter, open-label, randomized controlled trial. Ultrasound in Obstetrics & Gynecology 2016;47(6):674-679.
-
Shrem G, Nagawkar SS, Hallak M, Walfisch A. Isolated oligohydramnios at term as an indication for labor induction: a systematic review and meta-analysis. Fetal Diagnosis and Therapy 2016;40(3):161-173.
-
Rossi AC, Prefumo F. Perinatal outcomes of isolated oligohydramnios at term and post-term pregnancy: a systematic review of literature with meta-analysis. European Journal of Obstetrics & Gynecology and Reproductive Biology 2013;169(2):149-154.
-
Dashe JS, Pressman EK, Hibbard JU, et al. Society for Maternal-Fetal Medicine (SMFM) Consult Series #46: Evaluation and management of polyhydramnios. American Journal of Obstetrics and Gynecology 2018;219(4):B2-B8.
-
Kechagias KS, Triantafyllidis KK, Zouridaki G, Savvidou M. Obstetric and neonatal outcomes in pregnant women with idiopathic polyhydramnios: a systematic review and meta-analysis. Scientific Reports 2024;14(1):5296.
-
Fetal Medicine Foundation. Polyhydramnios Severity Classification Systems. London: FMF; 2024.
-
Abele H, Starz S, Hoopmann M, et al. Idiopathic polyhydramnios and postnatal abnormalities. Fetal Diagnosis and Therapy 2012;32(4):251-255.
-
Tsakmaki E, Ververi A, Chatzakis C, Cavoretto P, Sotiriadis A. Genomic abnormalities in apparently isolated polyhydramnios and the role of confirmed fetal phenotype: a systematic review and meta-analysis. American Journal of Obstetrics & Gynecology MFM 2024;6:101469.
-
Brzezinski-Sinai NA, Stavsky M, Rafaeli-Yehudai T, et al. Induction of labor in cases of late preterm isolated oligohydramnios: is it justified? The Journal of Maternal-Fetal & Neonatal Medicine 2019;32(14):2271-2279.
-
Leytes S, Kovo M, Weiner E, Ganer Herman H. Isolated oligohydramnios in previous pregnancy is a risk factor for a placental related disorder in subsequent delivery. BMC Pregnancy and Childbirth 2022;22(1):912