A patient Mrs. X, 20 years old,Primigravida came at North East Medical College Hospital with 38 weeks of pregnancy with obstruted labour with moderate anaemia on 15th December, 2024. On admission she was dehydrated, tacypnic, pulse 120/ bpm, blood pressure 120/70 mm of hg.haemoglobin 7 g/dL.
She was supposed to underwent Caessarian Section in a private clinic, but the anaesthesist and obstretician refused to do it in clinic because of her anaemia and unusually high pulse rate. They referred her to tertiary center.After initial resuscitation ceassarean section was done in NEMC hospital. The Baby was alive with low APGAR and patient’s recovery was smooth and uneventful. In first post operative day her all vitals were normal and she was given liquid diet and soft rice.
After 48 hours, on her second post operative day her abdomen gradually became distended, bowel sound became absent and suddenly she developped severe respiratory distress. The attending doctor tried with propped up position, oxygen inhalation and intravenous frusemide as it was taken as heart failure but patient was not improving rather became critical within an hour. She became tacypnic, respiratory rate 30 bpm and saturation dropped to 60%.
Then she was shifted to ICU on 17th December. That time her respiratory rate was 30/min, pulse was 120/bpm, blood pressure 110/70 mm of hg, temperature 99 degree fahrenheit , saturation 60%, abdomen distended.On
Auscultation breath sound was absent in left lower zone, diminished in middle and upper zone but normal normal in right side.
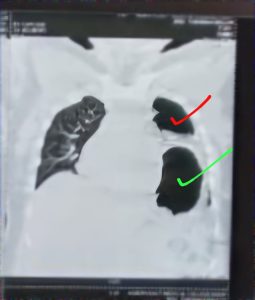
On the same day a portable X ray done that shows pnemothorax in left side.
Niddle was inserted in her lt second intercostal space, some air came out of the thorax and patient felt a bit better for sometime only. Again her distress increased which make doctors to bring a second differential diagnosis.
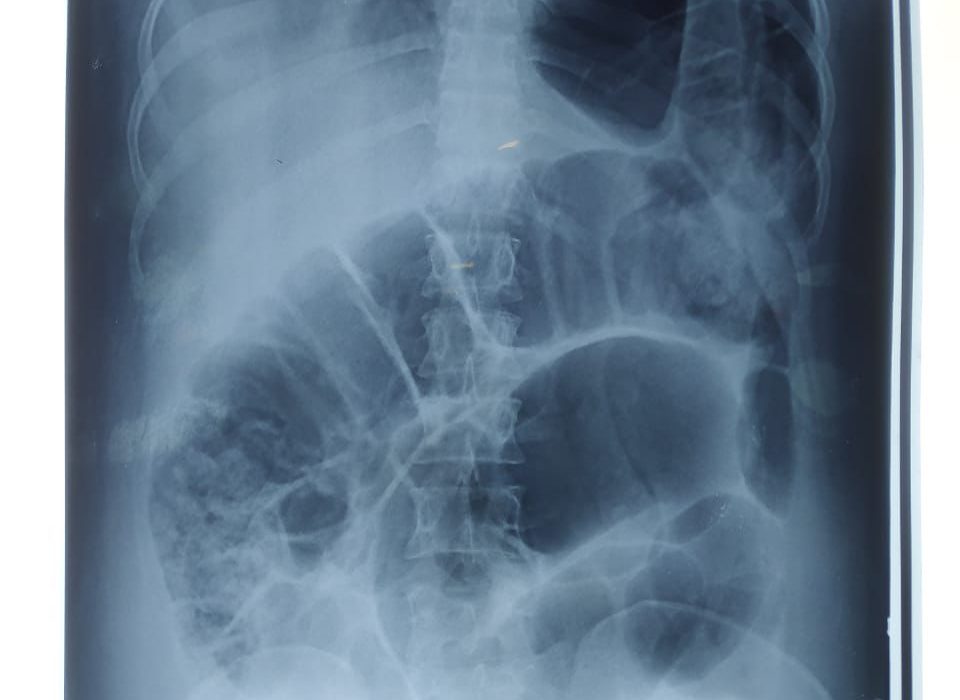
In next morning another X ray done in erect posture that shows hugely distended loop of gut in her left mediastenum that had pushed the left lung upwards.
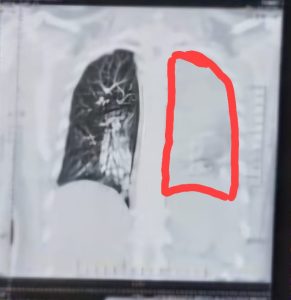
To support the X-ray, a CT chest done . CT report was as same as X ray. In some section of the CT scan lung tissue was totally absent and in some section lungs was confined only in apical region.
Bed side USG of chest shows decreased sliding movement in upper and mid zone in left lung, On rt side sliding movement was normal.a, but absent in lower zone. On rt side normal sliding movement.
Finally it was diagnosed as a diaphramatic hernia. Intestinal loops entered into the thoracic cavity and trapped. So her abdomen became distended, lung tissue compressed to the upper zone the left side.
Then she again shifted to Surgery department for repair of diaphramatic hernia. After repair patient is doing well.





1 Comment